Medical Mutual Claim Appeal Form . Medical mail this form to the address listed on the back of your member identification (id) card. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. Designation of authorized representative for appeals or to request information. The par form is used for all provider inquiries and provider appeals related to reimbursement. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. Check one type of request that best describes your. This form is only for appointing an authorized representative. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as.
from www.uslegalforms.com
Medical mail this form to the address listed on the back of your member identification (id) card. This form is only for appointing an authorized representative. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. Designation of authorized representative for appeals or to request information. The par form is used for all provider inquiries and provider appeals related to reimbursement. Check one type of request that best describes your. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use.
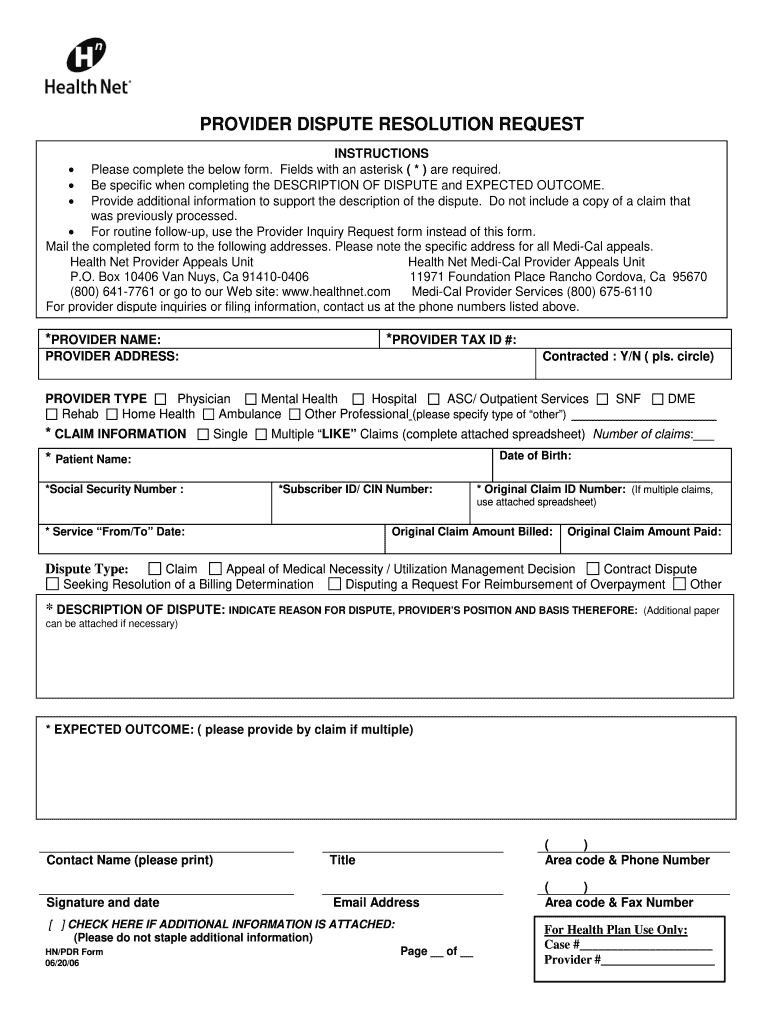
Health Net Provider Dispute Form Fill and Sign Printable Template
Medical Mutual Claim Appeal Form •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. This form is only for appointing an authorized representative. Medical mail this form to the address listed on the back of your member identification (id) card. Designation of authorized representative for appeals or to request information. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. Check one type of request that best describes your. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. The par form is used for all provider inquiries and provider appeals related to reimbursement.
From www.pinterest.co.uk
Sample Letter to Appeal a Medical Claim Denial Form Template in 2023 Medical Mutual Claim Appeal Form How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. This form is only for appointing an authorized representative. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. I confirm my wish. Medical Mutual Claim Appeal Form.
From www.sample-templatess123.com
Medical Claim Appeal Letter Sample Templates Sample Templates Medical Mutual Claim Appeal Form Medical mail this form to the address listed on the back of your member identification (id) card. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for. Medical Mutual Claim Appeal Form.
From etactics.com
5 Sample Appeal Letters for Medical Claim Denials That Actually Work Medical Mutual Claim Appeal Form Designation of authorized representative for appeals or to request information. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. This form is only for appointing an authorized representative. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to. Medical Mutual Claim Appeal Form.
From www.planforms.net
Physicians Mutual Insurance Company Dental Insurance Claim Form Dental Medical Mutual Claim Appeal Form •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. This form is only for appointing an authorized representative. The par form is used for all provider inquiries and provider appeals related to reimbursement. Check one type of request that best describes your. For a first level appeal, you. Medical Mutual Claim Appeal Form.
From www.claimforms.net
Medica Claim Adjustment Form Medical Mutual Claim Appeal Form Medical mail this form to the address listed on the back of your member identification (id) card. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. The par form is used for all provider inquiries and provider appeals related to reimbursement. Check one type of. Medical Mutual Claim Appeal Form.
From www.yumpu.com
Old Mutual Funeral Claim form Mymgf.co.za Medical Mutual Claim Appeal Form Check one type of request that best describes your. Medical mail this form to the address listed on the back of your member identification (id) card. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. Designation of authorized representative for appeals or to request information.. Medical Mutual Claim Appeal Form.
From allsopaiauthor.blogspot.com
How To Write A Claim Letter For Health Insurance Allsop Author Medical Mutual Claim Appeal Form The par form is used for all provider inquiries and provider appeals related to reimbursement. This form is only for appointing an authorized representative. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. I confirm my wish to claim from my health insurance policy and withdraw. Medical Mutual Claim Appeal Form.
From www.templateroller.com
Sample Appeal Letter for Medical Claim Denial Download Printable PDF Medical Mutual Claim Appeal Form Check one type of request that best describes your. The par form is used for all provider inquiries and provider appeals related to reimbursement. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. Designation of authorized representative for appeals or to request information. I confirm. Medical Mutual Claim Appeal Form.
From www.signnow.com
Medical Mutual Par 20172024 Form Fill Out and Sign Printable PDF Medical Mutual Claim Appeal Form Check one type of request that best describes your. Medical mail this form to the address listed on the back of your member identification (id) card. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. How does medical mutual determine if a new medical technology. Medical Mutual Claim Appeal Form.
From www.planforms.net
Unitedhealthcare Community Plan Claim Appeal Form Medical Mutual Claim Appeal Form The par form is used for all provider inquiries and provider appeals related to reimbursement. Check one type of request that best describes your. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. Medical mail this form to the address listed on the back of your member identification. Medical Mutual Claim Appeal Form.
From www.claimforms.net
Medical Mutual Claim Form Fill And Sign Printable Template Online Medical Mutual Claim Appeal Form This form is only for appointing an authorized representative. Designation of authorized representative for appeals or to request information. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. Check one type of request that best describes your. The par form is used for all provider inquiries. Medical Mutual Claim Appeal Form.
From www.planforms.net
Alignment Health Plan Provider Appeal Form Medical Mutual Claim Appeal Form For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. Check one type of request that best describes your. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. This form is only for appointing. Medical Mutual Claim Appeal Form.
From simpleartifact.com
Medical Claim Appeal Letter Template Examples Letter Template Collection Medical Mutual Claim Appeal Form Check one type of request that best describes your. For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. I confirm my wish. Medical Mutual Claim Appeal Form.
From simpleartifact.com
Medical Claim Appeal Letter Template Examples Letter Template Collection Medical Mutual Claim Appeal Form Designation of authorized representative for appeals or to request information. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. This form is only for appointing an authorized representative. Check one type of request that best describes your. Medical mail this form to the address listed on the back. Medical Mutual Claim Appeal Form.
From davida.davivienda.com
Claim Appeal Letter Template Printable Word Searches Medical Mutual Claim Appeal Form I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment from the. The par form is used for all provider inquiries and provider appeals related to reimbursement. Check one type of request that best describes your. Designation of authorized representative for appeals or to request information. This form. Medical Mutual Claim Appeal Form.
From etactics.com
5 Sample Appeal Letters for Medical Claim Denials That Actually Work Medical Mutual Claim Appeal Form For a first level appeal, you must send your appeal to medical mutual within 180 days of receiving your initial denial notice or as. This form is only for appointing an authorized representative. How does medical mutual determine if a new medical technology or procedure is covered?” we perform an extensive evaluation of the new use. The par form is. Medical Mutual Claim Appeal Form.
From www.vrogue.co
Medicare Appeal Letter Examples Amulette vrogue.co Medical Mutual Claim Appeal Form Designation of authorized representative for appeals or to request information. The par form is used for all provider inquiries and provider appeals related to reimbursement. Medical mail this form to the address listed on the back of your member identification (id) card. This form is only for appointing an authorized representative. Check one type of request that best describes your.. Medical Mutual Claim Appeal Form.
From etactics.com
5 Sample Appeal Letters for Medical Claim Denials That Actually Work Medical Mutual Claim Appeal Form Medical mail this form to the address listed on the back of your member identification (id) card. •any appeal and all supporting documentation must be received by medical mutual wellness by the appeal deadline in your program overview. I confirm my wish to claim from my health insurance policy and withdraw from my medisave to pay for my medical treatment. Medical Mutual Claim Appeal Form.